

Allergies are caused by an overreaction of the body’s immune system to substances that in most cases would otherwise be harmless
 Common triggers of respiratory allergy include pollens, house dust mites, moulds and animal dander. Inhalation of allergens can cause inflammation and symptoms in both the upper and lower airway. In the upper airways symptoms include allergic rhinitis (inflammation of the upper airways), conjunctivitis (itchy, watery eyes), and allergic asthma (inflammation of the lower airways).
Common triggers of respiratory allergy include pollens, house dust mites, moulds and animal dander. Inhalation of allergens can cause inflammation and symptoms in both the upper and lower airway. In the upper airways symptoms include allergic rhinitis (inflammation of the upper airways), conjunctivitis (itchy, watery eyes), and allergic asthma (inflammation of the lower airways).
These symptoms can worsen over time if not treated appropriately, and allergic rhinitis is considered to be one of the major risk factors in the development of asthma.
 Up to 500 million people suffer from allergy
Up to 500 million people suffer from allergy
The prevalence of respiratory allergic disease has increased over recent decades and is rising in both developed and developing countries. Globally, an estimated 400-500 million people are affected by allergic rhinitis and 40% of these are children.
It is estimated that 10-20% of allergic rhinitis sufferers have symptoms which are not well controlled despite the use of symptom-relieving medication and that less than one in ten of these receives allergy immunotherapy treatment.
A common comorbidity of allergic rhinitis is allergic asthma
 The duration and severity of rhinitis have a direct influence on the development of allergic asthma and the likelihood of recovering from it. Just like allergic rhinitis, allergic asthma is a condition that can be triggered by exposure to particular allergens, such as grass pollen, tree pollen, or house dust mites.
The duration and severity of rhinitis have a direct influence on the development of allergic asthma and the likelihood of recovering from it. Just like allergic rhinitis, allergic asthma is a condition that can be triggered by exposure to particular allergens, such as grass pollen, tree pollen, or house dust mites.
Whereas allergic rhinitis causes inflammation and irritation in the eyes, nose and the upper airway, allergic asthma primarily affects the lower airways. Symptoms of allergic asthma include wheezing, chest tightness, shortness of breath and persistent coughing.
Asthma development more likely among allergy sufferers
Studies show that allergic rhinitis and allergic asthma are closely linked, with nearly half of respiratory allergy sufferers experiencing both. Indeed, many people with allergic rhinitis go on to develop allergic asthma.
Treating allergy and asthma together
As a result, evidence increasingly suggests that, rather than being two separate conditions, allergic rhinitis and allergic asthma are caused by the same allergy and that treating – the allergy – can be beneficial for both conditions.
Allergic rhinitis negative impacts quality of life
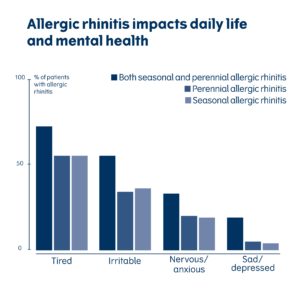 More than 50% of patients experience impaired quality of sleep because of their symptoms and 80% of patients report a negative impact on performance at work or school. In addition, it has been shown that co-morbid asthma reduces the quality of life even further and that the impairment increases with the severity of asthma.
More than 50% of patients experience impaired quality of sleep because of their symptoms and 80% of patients report a negative impact on performance at work or school. In addition, it has been shown that co-morbid asthma reduces the quality of life even further and that the impairment increases with the severity of asthma.
Millions of workdays lost
For many people, respiratory allergy has a significant impact on their quality of life, causing sleepless nights, shortness of breath and resulting in millions of lost school and work days.
What are the allergy treatment options?
Allergy immunotherapy treats the underlying cause of allergy and gives long-lasting improvement by reprogramming the immune system to better tolerate specific allergens. There are two ways of treating allergic rhinitis. Both have been shown to provide relief and put an end to discomfort and feeling ill.
 Symptom relieving medication
Symptom relieving medication
Symptomatic treatments are typically used to relieve the symptoms of allergic rhinitis but only work while the medicine is being taken. They have no long-term effect on the allergy itself. This is because, while they reduce the symptoms of allergy, unlike immunotherapy, they do not induce allergen tolerance.
Most symptomatic treatments are available over-the-counter (OTC), for example, in supermarkets or pharmacies, and include pharmaceutical medicines such as antihistamines, nasal steroids and decongestants.
 Immunotherapy treatment
Immunotherapy treatment
Immunotherapy treatment has demonstrated a long-term effect which offers a sustained improvement in the patient’s condition, sometimes for several years following treatment.
The main difference between symptom relieving medication and immunotherapy treatment is that immunotherapy induces tolerance and so alters the natural course of the disease. There are immunotherapy treatments available for each of the most common respiratory allergens.